A patient travels across the ocean to treat his cancer and get drenched in Mumbai’s first showers
“Hey, Bruce!” I exclaimed with surprise, a big smile on my face as I bumped into him in the hospital corridor during my rounds. At 6 feet 2 inches, he was hard to miss. He had a square frame upon which his broad shoulders rested. His brown French beard made its presence felt over his fair complexion. Even though he had a tough exterior, he had the kind of face that if you saw the first thing in the morning, your day went well.
“It’s so lovely to see you, buddy,” I said to all of his 72 years and all of his 72 hairs. He had been born in Zimbabwe, and after having lived on a few continents in his younger years, he had decided to settle down in a quaint town in southern Africa. “What brings you back to us?” I enquired. My orthopaedic colleague Dr. Mudit Khanna had done a knee replacement on him a few years ago with such astounding success that from not being able to walk a few steps he was cycling 30 km every day. I knew him well because when Mudit and I went to his country on a work visit, he took us both for a 4-hour cycle ride in the bush where lions roared not very far from us.
“I’ve been diagnosed with prostate cancer,” he said matter-of-factly, “and this is where I have faith, so that’s why I’m here.” Trust and conviction are so crucial in healing I thought to myself. As one of the greatest physicians of the 20th century, Sir William Osler, said, “Nothing in life is more wonderful than faith – the one great moving force which we can neither weigh in the balance nor test in the crucible.” “The urologist will do a biopsy and then plan ahead,” Bruce added, convinced he was going to be cured. “But before I start any treatment, I have a request. Let’s go for a bicycle ride around the city,” he said, clearly reminiscing the wonderful time we had had together. “Deal,” I confirmed, as we shook hands.
So at 6 AM on the following Sunday, Mudit and I picked up Bruce from the hospital. It was the first weekend that the city had been blessed with the onset of the monsoon. The three of us rode along wet Mumbai roads glistening from their first wash in the rain. The crisp air and cool breeze made the climb up Pedder Road seem like a walk in the park, and for Bruce the veteran, it was more of a saunter. We had decided to give him a cycle tour of the city, and as we rode past Marine Drive, we saw a bunch of overjoyed Gujrati adults indulging in garba, circling a loudspeaker in the pouring rain at 7 in the morning. Our day was made.
We rode past pigeons flying off near the Gateway of India and took pictures with the iconic Taj Mahal hotel as our backdrop. The skyline of the city looked so beautiful as raindrops peltered the Arabian sea. “This is such a great way to see the city,” Bruce was thrilled. “You get to see it from such a different vantage point – not too fast, not too slow,” he pondered completely soaked in the rain. After encircling 20 km of south Mumbai, we stopped at Cafe Mondegar for breakfast, and Mudit ordered a couple of beers for breakfast – because that’s what orthopaedics do. We fed Bruce some kheema pav to tickle his tastebuds; little did we realise that as an African, he had tasted the meat of nearly every conceivable animal. “Are you allowed to drink and ride in this city?” he asked. “As long as you don’t hit a bump and spill the drink, it’s fine!” I joked. We rode back via Kala Ghoda, Flora fountain, and CST station as the pelting rain stung us with pleasure in the face. It was an invigorating 40 km ride and an excellent start to the day.
Medical tourism is the practice of travelling across international borders to seek healthcare services. It was once a liberty of the rich, who travelled to the hot springs of distant Mediterranean countries to soak themselves in mineral rich water that had healing properties, or those who travelled from underdeveloped countries to developed ones for medical aid. Today, it is a common and an affordable affair for people in developed countries who are not that well-off to travel to developing nations offering the same medical care at reasonable prices and comparable expertise.
Every individual wants optimal healthcare for themselves and their families. Oftentimes, however, the care that one is seeking is not available within short distances. Occasionally, even when care is available, one might not be able to avail of it within the desired timeframe. The wait list for a knee replacement in countries like Canada and the United Kingdom, which follow a socialist practice of medicine, is over a year. In India, you could book a knee replacement as fast as you could get a burger from a drive-through at McDonald’s. And unlike McDonald’s, at some places, when you go in for a knee replacement, you can get the other one at half price.
Sometimes, the financial implications in the patient’s home country may be prohibitive. An uninsured US citizen was once treated at our hospital by me for a complex multi-level spinal fusion surgery that was to cost her USD 100,000 in her country. She had the same operation done by us here for one-tenth the cost and was so happy that she flew back business class! There is also a certain special doctor–patient relationship that develops when patients travel long distances to see a physician or surgeon; friendships are made, bonds are established, and families are extended. Metaphorically, not literally.
According to sources, India ranks at number 7 among the 20 wellness tourism markets, with over 56 million trips made to India for medical value tourism that generated USD 16.3 billion in revenue. It also ranks at number 3 in wellness-focused countries in the Asia Pacific, with Thailand leading the race. That may be because we offer only a bicycle ride as an additional service to our tourists!
Over the course of the next 10 days, Bruce completed his treatment. He looked well and rejuvenated. He seemed happy to have made the choice to come back to us at Wockhardt. “My doctors have given me permission to ride my bike as much as I can,” he said with glee, clearly not letting the diagnosis of cancer interfere with his joy of living. “Hakuna matata,” I told him, as we fist-bumped each other.
The stoicism of a 32-year-old woman battling two life-threatening diseases is a lesson in acceptance and courage
I did not know I was going to meet someone like her. She was all of 32 years old and sat in front of me with the poise of someone who had completed finishing school. Her white top enhanced her wheatish complexion. She crossed her legs one over the other with such elegance that even her linen pants did not wrinkle. Her ageing father watched her as she responsibly arranged all her files and papers on the table in front of us – the metaphysical barrier that allows a physician to maintain an emotional distance from their patient.
She had black wavy hair with streaks of silver. Her eyes seemed to have the accrued wisdom of several previous generations. Her face had the serenity of the Buddha and adorned a gentle compassionate smile. But the first words that came out of her mouth were earthshattering to me. “I have breast cancer,” she said with a composure I have never seen. From the corner of my eye, I could see tears rolling down from her fathers’ face. “In both my breasts,” she added stoically. “I’m so sorry to hear that,” I emphasized, “but what brings you to me?” the neurosurgeon in me inquired. “My oncologist got a PET scan done to plan the course of treatment and they found a tumour in the brain as well. That’s why he sent me to you,” she said. “We also got an MRI dedicated to the brain to ascertain what tumour it is,” she continued as she pulled out the films to show me.
“Aren’t you scared of all this?” I asked her, curious to know what was going on beneath that unflappable exterior. “I have loved the stars too fondly to be fearful of the night,” she smiled, impressing me with some Sarah Williams poetry. Literature is a great coping mechanism.
What was delivered to her was so unfair, I thought to myself as I plugged in the films one by one to analyse the scans. She didn’t have the slightest headache or, for that matter, any other symptom of the 6 cm ghoulish brain tumour nestled within her, between the frontal and temporal lobes in a region of the brain called the insula. After careful thought, I announced that this wasn’t a spread from the breast but a separate primary tumour of the brain. “This is a probably a low-grade glioma, a tumour that arises from the glial cells of the brain,” I decreed. “So, can we just leave it alone?” she asked with the curiosity of a child. “Can I proceed with the chemo and then go ahead with my mastectomy as planned by my doctor?” She told me she was eager to get back to flying as a pilot, and that she’d been granted leave only for three months. I didn’t have the heart to tell her that she might have to resort to a ground job in aviation.
Sometimes, there is no right answer. I thought for a while and explained that we would have to get rid of both tumours, and that we’d have to do them in quick succession. “We could do either of them first,” her oncologist told me over a phone call, “but if the brain tumour can wait, we’d rather do the breast,” he concluded.
I asked her what she would like to do. I remember my mentor, when faced with several options to choose from, always chose to tell his patients, “Whatever decision you make will be the right one.” I have religiously followed that practice over a decade. Except, I end up saying it more to my wife than to my patients.
“Let me get done with the breast and then we’ll proceed with the brain,” she decided together with me. I sat there in awe of her fortitude to take life-altering decisions with such surety although I was sure that a deluge of emotions might be erupting within. I find it tumultuous to deal with a flu, and yet, I see myself giving hope and strength to patients with brain and spine tumours on a daily basis. We bid adieu with a plan to operate on her head once she had gone through a mastectomy and breast reconstruction. Chemotherapy was to start in a week. Yes, oftentimes in the treatment of cancer we need to administer chemotherapy to shrink the tumour before we operate on it.
Two months later, her father called frantically saying that she had had a seizure. She was unconscious at home. They took her to the ER of the closest hospital, which managed to salvage the situation. The day of the seizure was the day she had completed her chemo, and she was scheduled to undergo breast surgery a few days later. However, a repeat MRI of the brain showed that the brain tumour had grown marginally. We had a muti-disciplinary tumour board meeting and decided to go ahead with the brain surgery first. A couple of days later, we opened up the head to enter an area that was once known as ‘no man’s land’; such was the danger that surgeons used to avoid going there. It was like the Kashmir of the brain: difficult to access, but once there, it enraptured you. We strode in bravely and could remove the entire tumour as it was, straddling the areas of cognition, motivation, fear, anxiety, and happiness. She woke up smiling broadly – a rarity after brain surgery. We discharged her in a few days fit enough to have her second operation. Weeks later, she called to tell me that recovery from her brain surgery was a walk in the park compared to a double mastectomy with breast reconstruction. “We only dug a hole; they resurrected a whole new structure,” I facetiously justified the hard work of my colleagues.
The Financial Times recently published an article on the unexplained rise of cancer among millennials. It mentioned that the past 30 years have seen an upsurge in cases of so-called “early onset” cancers in the under 50s. So marked is the increase that leading epidemiologists have suggested it should be called an epidemic. Scientists are not sure why, but changes to nutrition and ways of living hold at least part of the key to the puzzle. The consumption of food high in saturated fat and sugar is believed to alter the composition of the protective gut microbiome in ways that can harm an individual’s health. Excess usage of antibiotics and other medication may also be responsible for altering the gut. Whether it will happen to one of us, only time will tell; now, it is also possible for us to do a whole genome sequence analysis to check if we could be at risk. “Our graces don’t stand to reason any more than our sins do,” I read on someone’s Twitter handle.
She returned three months after having valorously completed both her surgeries. Her long hair had transformed into a small frizzy bun, gracefully sprouting again after being jettisoned by the chemo. There was no tumour in the brain and the breasts were brand new. She beamed with confidence, hugging me tightly.
“When can I start flying?” she asked like a little child eager to return to her playground. Knowing that this was a permission I couldn’t grant as yet, I replied, “You’re already soaring way above everyone else.”
The real test of courage occurs when a loved one is on the brink of life and death. How do we then deal with the ultimate truth that life is unpredictable?
A couple of months ago, I was demonstrating a surgical procedure live at a conference. A colleague and I were exhibiting how to perform a minimally invasive spinal fixation in a patient with degenerative instability of the spine. The surgery was being telecast live to a conference room where a receptive and enthused audience had gathered. It was simultaneously being broadcast online, where a few hundred people were attending. Besides the usual surgical paraphernalia that adorns someone who operates, we were hooked on to mics where we could explain to the audience what we were doing and answer questions related to our decision making, technique, and nuance. The crowd was replete with resident doctors and junior and senior colleagues, all of whom watched our every move with a hawk’s eye. Being part of a scenario like this can be unnerving, but I am surprisingly comfortable with this mode of teaching; we regularly have observers and visitors in our operation theatres from other institutes whom we are happy to teach.
Just as I completed inserting the final screw to complete the procedure, the anaesthetist tapped me on my shoulder, signalling that I should step down from the platform I was standing on. She asked the audio–video guys to turn my mic off and indicated to my colleague to continue with surgery. I was temporarily perplexed. I was sure I hadn’t done anything silly, and I double-checked to confirm that the patient was stable. We were just about to conclude a perfect operation I was proud of.
She took me to the side and in a very maternal voice whispered, “Your father has just had a heart attack.” “My father?” I questioned, not from fear or panic but simply from disbelief that such a robust, energetic, and one-in-a-million man would fall prey to a such a mundane condition. “He had severe chest pain which has gotten better with sorbitrate, but they have ordered cardiac enzymes and are planning to do an angiogram,” she concluded. “So how do we know it’s a heart attack?” I asked, with only half the information available to us. “You should just go,” she reasoned.
My father is a surgeon too and was in his hospital when it must have happened, so I knew he would be well taken care of. I removed my gloves and gown while my colleague completed the last bit of the procedure. Once I got hold of my phone, I was assured he was conscious and fine as they wheeled him in for an angiogram. I gave verbal consent to his team to go ahead and do what they deemed fit.
I drove two hours from the grubby suburbs of Mumbai into town where he was. As I restlessly manoeuvred though horrendous traffic, I pondered about the shortcomings of life. The magnitude of the adage ‘how unpredictable life is’ begins to dawn on you only when it strikes home and affects your own blood. As neurosurgeons, no one is more prepared for uncertainty than we are, but just as we begin to tell ourselves we’ve seen it all, life throws us another curveball. Half an hour and only half a kilometre later, I was informed that the angiogram was normal and that he didn’t need a stent, but he would need to be started on blood thinners as his cardiac markers were marginally elevated. He hadn’t had a heart attack after all. By the time I finally reached, he was lying comfortably in the ICU and sipping tasteless hospital chai, showing family and friends his biceps at the age of 78.
Cut back to a couple of weeks ago. My mother had travelled back from London via tiring connections on a Saturday afternoon. We stay in the same building; she is on the third floor while I’m on the ground. When I went to see her early in the evening, she was resting in bed. “I’m very sleepy, I’ll talk to you later,” she turned on her side and buried her head into the pillow. One hour later, her house help rings my door bell slightly worried, “I’m trying to wake up madam to give her tea but she’s not moving,” she said in Hindi. “She’s not eaten anything since she came back,” she continued, trying to give me some context. I rushed up to see her and was shocked at what I saw.
My mother was breathing heavily, almost grunting. Her tongue had rolled back in her mouth, obstructing her airway. Her eyes were roving in all directions. “Mom!” I shouted, slapping her face like they do in the movies. I dug my fist into her sternum to see if there was any response to pain. None. I shone my phone torch in her eyes, thankfully noting that her pupils were reacting well. That meant she wasn’t brain dead. I had to quickly transition from thinking like a son to behaving like a doctor. I turned her to the side and made sure her airway was protected. “This could be a stroke or a massive bleed in the brain,” I thought to myself, having seen thousands of patients who have looked exactly like this. But I also know she’s diabetic, and the first thing to do in anyone with altered sensorium is to check their sugar. I was aghast to see that it had plummeted to 30, where the normal range is 80–120. This was dangerously low. She was in a hypoglycaemic coma and all I needed to do was to get sugar into her system but there was no way to do it orally.
I had two options: I could either run to a chemist and get an intravenous cannula, tubing, and dextrose or I could take her to the hospital, both of which would take me 20 minutes. She was on the brink of life or death, and the decision I made could decide which side she rolled over on. A thousand thoughts ravaged my mind. What if the chemist doesn’t have everything I need and I’m not able to get the sugar into her on time? What if it’s something more than just hypoglycaemia and she needs a scan of the brain? What if I’m late in getting her to the hospital and she sustains irreversible brain damage? I have seen this myself, patients lying vegetative in a hospital bed for months because they took two hours to get to the hospital while in their prolonged hypoglycaemic state. I resolved to take her to hospital. Hustling an ambulance would be a waste of time, so I emergently called my wife and along with the house help, lugged her lifeless body off the bed, into the elevator, and then dragged her into the backseat of the car. She was 70 kilos of dead weight. We drove to my hospital and everyone in the ER was ready to receive her. We started an intravenous access, pumped in the glucose, and within 40 minutes of my seeing her almost dead at home, she gently started bouncing back to life as the sugar kickstarted her system that was dependent on it.
“What’s happening?” she asked in a daze, confused by all the pandemonium around her. I explained briefly but I don’t think she registered any of it. We got an MRI done do ensure there was no permanent damage from the hypoglycaemia and to rule out any other calamity. She was transferred to the ICU for overnight monitoring. When she was coherent, she explained that she had taken her regular dose of insulin but didn’t end up eating as much amidst the layovers and jet lag. Gratefully, we went home walking the next day.
In a span of three months, both my parents transiently made a brief sojourn towards heaven but returned to us briskly. Through it all, the uncertainty and unpredictability of life that we are often reminded of – but regularly disregard – oscillated in front me as I swayed from doctor to son and back. Scared. Strong. Solaced.
Medicine is all about uncertainty, with neither diagnosis nor surgery or the process of recovery offering any guarantees
There are some patients in whom you can make a diagnosis the moment they saunter into your clinic. Sometimes, it’s in the way they walk, either in their limp or the way they get into their chair. Sometimes, it’s in the hand they prefer to use to pull out their papers. Occasionally, it’s in the way they greet you – the intonation of their voice, the sound of their speech, the tilt of their head. In the first few minutes while a patient is settling down to narrate their story, a physician is accruing their compounded wisdom of the patients they’ve seen over the years to decipher what the problem is. There is an innate tendency in a doctor that prompts them to evaluate themselves before they evaluate the patient. Unless you’re a bariatric surgeon, where diagnosis isn’t much of a challenge; in neurosurgery, the possibilities are numerous.
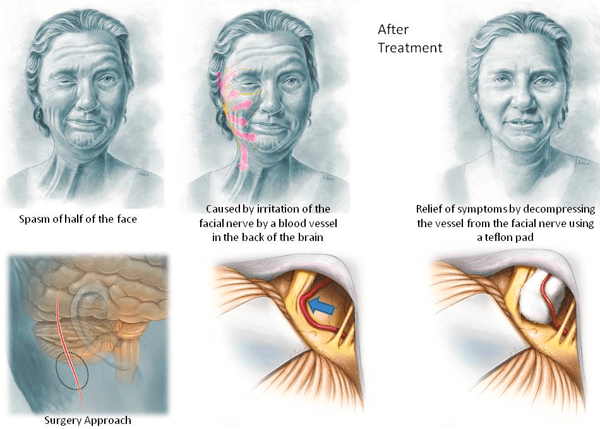
The diagnosis is often challenging, but like in the case of Mr. Joshi, it was staring me in the face – quite literally. The right side of his face was twitching incessantly. The forehead jumped as if it wanted to leave his body, his eye fluttered in a staccato fashion, the cheek was reverberating, and the angle of his mouth moved like it was dodging bullets. The left side of his face was placid and stayed still, a silent observer to the cacophony of its other half. He used his hands with futility to try and stop these involuntary movements so that he could start talking. It was one of the most severe forms of a hemifacial spasm I had seen in my life. Most patients have much milder versions of this, with a twitch here and a twitch there.
Nikhil Joshi was a retired insurance agent in his early 70s who had been plagued by this problem for over a decade. He wore a crumpled white shirt that was half tucked into his loose grey striped pants and carried a khaki bag, a look that some creative geniuses like to carry. His stubble was uneven too – the contracting muscles of his face must have made it hard for him to shave on the right – which only further typified the creative look. “He finds it exhausting even to make conversation,” said his wife sitting next to him, agonized. “Brushing my teeth, chewing my food is also very difficult,” he spoke for the first time, his voice transforming into a stammer from the twitching. Air escaped from the angle of his mouth, further muffling the sound.
“Do you feel any pain?” I asked and he nodded his head sideways to say no. I wanted to differentiate it from another separate entity, where patients have sharp shock-like sensations over the forehead, cheek, or jaw but without a spasm. We call that trigeminal neuralgia, where the sensory nerve to the face is compressed by an artery or vein in the back of the brain. In Mr. Joshi’s case, it was his facial nerve, the nerve that controls the motor function of the face, which was being distorted by the constant pulsations of a large tortuous vessel pounding on it. I plugged in his MRI to show him the problem. He was aware of it but was scared to have an operation, which would entail mobilizing the artery from the nerve such that there is no conflict between the two. It’s the same thing I do when my 7- and 9-year-old daughters fight: make space for them. Adopting surgical strategies to parenting is my thing.
“I have tried lots of medication but it hasn’t helped,” he said, as I struggled to decipher the words coming out of his mouth. “Someone told me to even try marijuana, which I did, but it was of no use,” he confessed. “Have you tried Botox?” I asked; Botox, when injected at a different dose from that used by women as face fillers, can relax the muscles of the face, providing some relief. “Five times in ten years!” his wife answered. “It improves the condition very little, as it works for a few weeks and then it’s back to normal,” she spoke for him.
“I think we should try and eliminate the root cause of the problem,” I said, trying to broach the real issue, “and that, I’m afraid, only surgery will do.”
“Guaranteed?” he asked, nodding his head in the way Indians do whilst seeking an affirmation. “I can give you a guarantee of more than 90%,” I told him, as if we were striking a deal. “The 5-10% that remains will depend on how much the covering of your nerve has already been injured by the constant hammering,” I said, to cut myself some slack, adding, “and also, you have to leave something to God,” I looked straight at the three ashen lines on his forehead. He agreed to that with folded hands. “Yes, sir. Yes, Sir,” he acknowledged God fearfully.
The thing about medicine is that all patients want certainty, but medicine is all about uncertainty. The human body is both simple and complex in simultaneity. Exactly the same surgery performed on different patients often yields varying results – unless you’re an obstetrician conducting deliveries. This is hard for patients to understand and doctors to accept.
A week later, he was under anaesthesia. We made a small incision behind the ear and drilled out a coin-sized piece of bone. I cut the dura covering the cerebellum and softly retracted it after releasing brain fluid, which would lighten the pressure inside. I zoomed the microscope smack onto the facial nerve after meticulously dissecting the web-like strands that traversed the blood vessels. There was an abnormally large artery grooving against the shoulder of the nerve and lifting it up, with another smaller one coursing through and through the nerve. “I can imagine why this guy’s face was gyrating away like that,” I told my colleague. We mobilized the artery from the nerve, and as I held them apart, my colleague perfectly placed a piece of fluffy Teflon between them, which served as a padding to keep them from touching each other. We did the same with the other smaller vessel. “I’m happy with this, are you?” I confirmed with him to check. “Yes,” he said unflinchingly, and so we closed.
When we wheeled him into the ICU after he had woken up, I went to check on him. I was a little shaken to see that his spasms had gotten worse. His eye would not open and his mouth would not move. The twitching persisted; in fact, it was even more rampant. Most patients have complete cessation of the twinge almost immediately after surgery. A zillion thoughts crossed my mind. The family was suspicious of my 90% guarantee. I went back and analysed my surgical video and confirmed I had done a perfect operation. It has happened to me once before where I had decompressed the incorrect nerve and had to go back the next day and rectify it. It’s a nightmare for any surgeon.
I appeased the patient and the family to hold on a little. By evening, the eye started opening. The speech returned. The spasms were down by 50%. The next morning, they were gone, never to return. For the first time in ten years, he was able to smile symmetrically. We still don’t know why some patients recover almost immediately after this surgery and some take a few weeks or months, while very few don’t improve at all. And that is why medicine is so mesmerizing.
He returned two weeks later to remove his sutures. Clean shaven. Ironed shirt, neatly tucked in. Tighter pants. The same khaki bag, though. “Thank you for saving my face,” he said profusely. “Now don’t come back shaking something else,” I joked with him as we hugged each other good bye.
“Mama and me are going to Mount Everest with a bunch of friends,” I told my daughters. This was after 22 of us, aged 16-60, had finalized a plan to trek up to Everest Base Camp.
“Isn’t that the tallest mountain in the world?” my 9-year-old asked. “That’s why we’re going, but we’re going only to the bottom of it,” I replied, and saw a very unimpressed look on the face of my 7-year-old. “Why would you take 10 days to reach the bottom of the mountain?” she enquired, probably slightly concerned that she’d have to be without both her parents for that long for the first time ever. “Because we have to climb more than 5000 meters, and one meter is roughly how tall you are, so imagine 5000 of you stacked up on top of each other!” I gestured, confusing her ever more. “And there’s less oxygen in the air at that level, so it’s hard to breathe and it’s also freezing cold,” I cuddled her tight trying to justify to her that what we were going to do was pretty valiant and she should be proud of her parents.
“How many people go this base camp every year?” she questioned further to crosscheck if what we were embarking on was really that big a deal. I quickly looked it up and announced that about 40,000 people do it annually. “How many people go to the actual top of the mountain?” her calculating mind asked. “Around 500,” I replied. She raised her eyebrows at me, clearly believing that she’d proved her point that what we were setting out for was simply a high-altitude picnic.
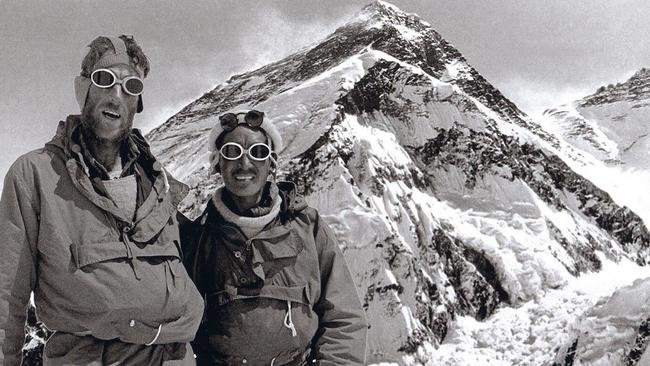
As I continued scrolling for more trivia, I was surprised to find out that fewer than 7000 people have summitted the top of Mount Everest (8848 m) in the 70 years since it was first scaled by Sir Edmund Hillary and Sherpa Tenzing Norgay on May 29, 1953.
So, in remembrance of its 70th anniversary, a month earlier on April 29, 2023, about two dozen of us set out to get to the top of the bottom of a mountain. An early morning Air Vistara flight took us smoothly away from the dusty suburbs of Mumbai and planted us in breezy Kathmandu. We were greeted at the airport by an ornate statue of Lord Buddha, which said, “Welcome to Nepal, the birthplace of Lord Buddha.” Until this point, I had always thought the Buddha was Indian. But how does it matter; he transcends these imaginary boundaries made by man and his teachings are universal.
THE DEATH RIDE
The next morning, we were scheduled to take a 30-minute flight from Kathmandu to Lukla (the starting point of the trek) but were informed that our flight was diverted to Ramechhap Airport, which is a 5-hour drive from Kathmandu.
So, at about 2 AM, we huddled into 2 minibuses and were driven along the craziest serpentine roads with the largest potholes by drivers unaware of an entity called death or motion sickness, even as one half of our group threatened to puke on the other half. We drove along the edge of a cliff yawning into the valley, with one half of a bus tyre constantly threatening to roll over. I couldn’t help but remember Hunter S. Thompson who famously tried to describe the edge, himself confessing that “There is no honest way to explain it because the only people who know where it is, are the ones who have gone over.” We were mentally prepared that we were flying to the most dangerous airport into the world; we just weren’t prepared that the road to it was also the same.
We arrived at Ramechhap as if we had come back from war, battle weary. The airport was four concrete walls open to sky and two rooms. Hordes of trekkers with their multicoloured backpacks converged in chaos to make their flight.
THE FLIGHT PLIGHT
We were booked on Sita Airways. And that’s where our Ramayana began. Every other plane took off apart from ours. Our flight, which was via a 14-seater plane, was overbooked, is what we were told. Who overbooks a 14-seater? We then got inside information that a group of international trekkers had paid the airlines more and so we were offloaded. By the time it was our turn to fly, the pilot had overflown his hours for the day. Our flight was supposed to be only 14 minutes long, but no exceptions were made.
By noon, the airport wore a disserted look. We took a stroll on the runway with a security guard who empathised with us. Parts of the airplane were dismantled in front of us for oiling and greasing, clearly indicating that we weren’t going to fly out from there that day. Driving to Lukla meant travelling on the edge of another cliff for 20 hours, which the group vetoed. We found accommodation in a guest house nearby and played volleyball with the locals instead, hoping to take the first flight out the next morning.
We walked over to the airport before sunrise but received news that the weather was not going to allow us to fly. Grey fleecy clouds had descended upon the mountain range, hanging over its neck like a sword. We coyly requested our pilot to take the risk, as we had already lost a day. Instead, he showed us a few YouTube videos of planes crashing into the mountains while trying to land at Lukla Airport.
Surrounded by several 7000-meter-tall peaks, it is not without reason Lukla is called the most dangerous airport in the world. The strong winds and thin air make it harder for the engines to generate thrust. Additionally, there are no radar or navigation systems at the airport, so pilots are fully dependent on what they can see from the cockpit. Also called the Tenzing-Hillary Airport and built by Hillary himself with the local sherpas, the runway is only half a kilometre long and inclined at a 12-degree slope. We agreed it wasn’t worth the risk even if it was the ‘runway on the roof of the world.’ “You can only go to the mountain on her timeline, not yours,” my wife said, trying to appease our impatience. I wondered who had assigned the feminine gender to a mountain.
A few hours later, the weather cleared up and one flight with half our group took off, with them sending pictures to those of us on the ground. We saw their broad smiles in the pictures they sent us from their twin-seater airplane, until they realised that the weather Gods had changed their minds a few minutes before they could land at Lukla and they had to take a U-turn mid-air to return to us, thankfully alive. It was gloomy once again. According to neuroscience, bad weather makes us turn inward and invites us to think more deeply, more clearly. We sat down to renegotiate our strategy over a few beers. Some of us were willing to shift the trek to Annapurna Base Camp. Our guide told us that while that was more scenic, the trek could also be full of leeches; I was unsure if our blood being sucked out was the scene he was referring to. Others were resolute about making it to Everest because it was a dream they had harboured for years. I, like for most things, didn’t have an opinion; I was just happy to be that high above sea level.
I remembered the American poet Ada Limon’s stunning poetry. “We’ve come this far, survived this much. What would happen if we decided to survive more?” I thought this poem would come to mind towards the end of our journey, but here I was, thinking of it at its very beginning. We were drained waiting for over 48 hours for a 14-minute flight, but we decided to brave one more night. The next morning, as the clouds lifted their veil over the brown mountains, we were on the first two flights of Sita Airways – Ram bharose.
It was a perfect touch-down at Lukla Airport, as the plane came to a halt 2 feet short of where the runway ended. A security guard pretended to screen our luggage as it was handed over to us. We had the famous trekkers’ breakfast at the damp and musty Buddha Lodge, stacked up on water, and started walking amidst planes taking off and landing at arm’s length.
THE FIRST WALK
Our first destination was a 4-hour walk to Phakding, a name that brought a mischievous grin to anyone who said it. We walked through the town of Lukla bumping into dzos, an animal that’s a hybrid of a yak and a cow as little school kids in blue uniforms, with pink cheeks and well-oiled hair, effortlessly strutted down the rocky steps that we were gingerly navigating.
We came across large boulders with Buddhist inscriptions. “You must always walk around these clockwise,” one of our guides, Shyam, told us, and we circumambulated in the right direction. He was in his mid-fifties and had been to Everest Base Camp over a hundred times. He looked like a younger brother of Om Puri, with his mottled face, but had a silken voice that gently prodded us to keep walking. We bumped into haggard trekkers who were returning from base camp, some of them looking like their noses were going to fall off, most of them parched from the sun and the cold. “It’s hard as hell, but definitely worth it,” most of them said, breathing heavily when I asked them how it was, with one solo trekker confessing, “I cried the last three days.”
We walked along a turquoise river as it bounded enthusiastically over granite boulders. There was a freshness, a sense of being undistracted in these spaces. The sight of a verdant expanse below and snow-capped mountains in the distance took away the weariness of walking, and we finally made it to our lodge in Phakding. We had dal and rice (our every meal over the next 10 days) and tucked ourselves into rooms separated by cardboard partitions, through which you could hear your neighbour breathe, let alone listen to everyone’s uncensored conversations.
THE FIRST CLIMB
The next day I awoke at first light and washed my face and brushed my teeth with water so cold it stung. When we assembled for breakfast, we bumped into Poorna Malavath, a 22-year-old girl from Telangana, who was the youngest girl to summit the top of Mount Everest just before she turned 14. At 22, she was now guiding an expedition to base camp, with one member of her team aged only 9. I, at 42, could only stare at her in disbelief and awe, even more fascinated by the human spirit. She later told us that she has summitted the tallest peaks of all seven continents. “The first step is the most crucial,” she said, as we parted ways to continue the second leg of our journey to Namche Bazaar, a 10-hour climb.
The clouds had made way for a blustery day, the sun shining bright on us, as countless vistas of the monumental mountains interspersed between deep ravines and several footbridges made way for some spectacular views completely enrapturing me. I couldn’t help but gawk in reverence for the sherpas who carried logs of wood, cylinders, crates, and other unimaginable loads on their backs, some of them doing so with cigarettes in their mouth. “Won’t smoking make it harder for you to breathe?” I asked one of them in Hindi, as he took a break for a puff. “This is medicine for altitude sickness!” he quipped back to regale us. “Plus, it keeps you warm,” he added, and marched on at 3000 meters.
Acute mountain sickness can occur if you ascend above 2500 meters. I later found out that the people of Nepal have different DNA than lowlanders that evolved via natural selection over centuries, enabling them to live comfortably at high altitudes. Their DNA contains DNA from Denisovans, one of the early hominins that interbred with Homo sapiens. To survive altitude sickness, one of our Gujju groupies had made camphor potlis for all of us to tie around our necks and inhale from deeply, as it was too late to interbreed with someone who had Nepali DNA.
“Anyone can develop altitude sickness,” Shyam explained. “It doesn’t matter how fit you are.” He went on to narrate the story of how, in 2010, Martina Navratilova at age 54 developed pulmonary oedema while attempting to climb Mount Kilimanjaro in Tanzania and had to be brought down immediately and hospitalised. I took two extra puffs of the camphor after listening to that, and soon thereafter we stopped for lunch to devour some more dal and rice, preparing for an even more uphill climb, which was both metaphorically and literally breath-taking. The steps became steeper, the climb harder.
“I try to best explain,” our other guide, Dinesh, started speaking with us in broken English, practising it with us to master it for his foreign clients. He was a lean and lanky chap who had completed his mountaineering training, but domestic responsibilities kept him from leaving for long expeditions and he had to resort to being a guide for treks to base camp. “There are five rules to climb the mountain,” he elaborated as he saw us pant. “Eat well, sleep well, drink well, walk slowly, and strong mind,” he concluded simply. I focused on number four, soaking in the sun before it set as we finally reached Namche Bazaar.
Namche is a pretty town with enormous rotating prayer wheels greeting us as we entered. It’s also a party town situated on the slope of an arch-shaped mountain, with amazing views of giant Himalayan peaks from anywhere in the valley. Little children ran all over, flashing their enormous fuchsia smiles.
Some of our boys slugged on beer at the highest Irish Pub in the world, while others strolled the market for more mountaineering gear. Multifarious shops lined cobbled streets running up and down the hill. “This town is famous for yak cheese and butter,” Shyam told us, “but it’s actually the female, called a dri, that gives the milk that produces all this,” he said; the yak refers only to the male. “Even in the animal kingdom, the males want to take credit for everything that the females do,” I pronounced as we sipped on coffee made from ‘yak’ milk at the Stupa Café that marked the entrance to the town.
We spent the night at a French-sounding teahouse called Camp De Base, and had our dinner at Thokathok restaurant. I don’t know what that word means in Nepali, but in Gujrati, it’s surely not a place to dine at! As Namche is situated at around 3500 meters, we had a reserve day here to acclimatize and were told we could walk up to the glorious Hotel Everest View (built by Takashi Miyahara, a Japanese-born tourism entrepreneur) for breakfast to get our first glimpse of the mountain, but it was pouring and misty and foggy and hazy, and hence we stayed in to have the last hot water shower of our trip.
THE FIRST GLIMPSE
After Namche, scarcity hits the mountains. Green slowly turns grey. Bushes make way for gravel. The price of mineral water goes up by a hundred rupees every 500 meters. There’s no wi-fi, no network; you can barely charge your phone. There is no heating and temperatures rattle around 0 degrees Celsius. Most lodges don’t have attached bathrooms. I remember washing my bum once with water so cold that everything I thought was supposed to come out went right back in, refusing to venture out. And they tell me that the outside of a mountain is good for the inside of man. I reminded myself that my goal in life was not to be more spiritual but to be more human.
The Nepali name for Mount Everest is Sagarmatha, meaning ‘the head in the great blue sky’, and the area we were trekking in was the Sagarmatha National Park. The next three mornings, we walked to the towns of Tengboche (3867 m), Dingboche (4410 m), and Lobuche (4930 m). I wondered why all these names ended with ‘che’; perhaps the Gujjus had settlements here even before the Nepalis arrived.
On the first of those three mornings, on Buddha Purnima, as the full moon made its way for an even fuller sun, we got our first glimpse of the top of Mount Everest, with the sky’s golden light bouncing the snow off it in tiny puffs. It was simultaneously majestic and simple. Beautiful and brutal. It merged into the landscape with humility and yet stood out with hubris. It swept you off your feet while firmly rooting you to the ground beneath. It stood in the way and yet it was the way. It synchronously both discarded and illuminated the notion of heaven. It was both the portal to the sacred and the profane. It was both the cacophony and the stillness. I wondered what Edmund Hilary must have felt to be the first to summit the mountain. I wondered what he must have felt when two decades later his wife and daughter died in a plane crash in the Himalayas.
Over the next three days, we continued to walk and climb arduously at the deepest yearning of our paradisal pursuits, watching the clouds floating like soft feathers jumping from one mountain to another. Shyam constantly chanted, “Slowly, slowly…” in the background, which, in his graceful intonation, urged us to move faster. In the days we spent together, he told us the story of how a group of ladies from New Zealand, all above the age of 60, have visited him over 10 times to trek in different parts of Nepal. All of them retired nurses, they run a free medical camp in his village as a gesture of gratitude every time they come.
THE ONWARD JOURNEY
We passed by tiny stupas with meditative Buddha eyes engraved on them and tombstones built in honour of the people who had succumbed to the mountains. Bright prayer flags adorned the little settlements along the way, snapping away in the brisk wind. “The blue colour is for the sky, white is for the wind, red for fire, green for vegetation, and yellow for the earth,” Dinesh told us, as we became more rooted with the elements amidst fellow trekkers that appeared more languorous than when we started.
We knew we were walking really high when there were choppers flying below us, airlifting people who were getting sick or those who just could not move any further. “The more you try to avoid suffering, the more you suffer,” I remembered Thomas Merton, as I saw a 12-year-old hooked onto an oxygen tank being helped by his team to reach the helipad.
We stayed the nights at modest accommodations where we overdosed on mountain whisky – a combination of ginger, lemon, and honey in hot water to warm our inners, while our outers gently shrivelled away. Shafts of sunlight streamed in through the foggy windows to awaken us in the mornings. It was both exhilarating and exhausting at the same time to be in the midst of ethereal beauty through the hardship. As Leonard Cohen put it in one of his finest songs, we’re “none of us deserving of cruelty or the grace.”
I felt my blood freeze in my veins at -15 degrees Celsius when we reached Gorakshep (5164 m) three days later, where a notice at the entrance of the town said, “There is no reliable water resource around, therefore we cannot provide drinking water.” We got ourselves mineral water at Rs. 500 a bottle.
FINALLY, EVEREST
Everest Base Camp (5364 m) was now just three hours away. We could see in the distance a snow-covered glacier speckled with yellow, blue, and red tents. After three days of perfect weather, once again, there was a large cloud cover looming over us. We marched on with renewed vigour and rigour, safely leaving it behind in the distance, and the sky miraculously opened up for us. We paraded on gravel and roved on rocky terrain as we finally reached our destination in the gathering chill of the early evening. The bean-shaped boulder that has Everest Base Camp graffitied on it with red spray paint, alongside numerous inscriptions of people’s signatures demonstrating a sense of been-there, done-that. It’s quite ironic that you can’t really see Mount Everest from Everest Base Camp, and that only the top tenth of it is visible on your way there and back.
We jumped atop the boulder and did all the routine touristy things like taking pictures by thumping our chests and pumping our fists. I had a premonition that a group of people would walk out of their tents and invite me to join their expedition to the very top of the mountain, but that thought quickly vanished when I remembered the story of a surgeon who summitted the peak but lost all his fingers to frost bite on his return.
Even though we returned from the base camp valiantly that evening, our journey wasn’t complete. Some of us had planned to scale Kala Patthar (5645 m) to watch the sun rise over Everest. It is from the top of this mountain that you can see a third of Everest. So, the next morning at 3 AM, wearing 4 layers of clothes with headlights strapped to our foreheads, we started the ascend amidst a starry silhouette of snow-capped mountains. As the sun began to rise a few hours later, a silver hue outlined the plethora of peaks that ensconced us.
“I can’t feel my toes,” my friend told me as we took small steps in the dark, breathing twice as hard. “Just wiggle them a little,” I joked, but after a few minutes he mentioned he couldn’t feel half his foot. He realised that discretion was the better part of valour and decided to descend. When he reached down, I was told his feet were purple; if he hadn’t decided to turn back then, he would have needed an amputation.
A few of us continued to ascend, placing our feet precariously to avoid slipping on the snow lining the rocks. As the sun loped upwards, the mountains changed colour from crimson to golden and then brown. I dared to remove my gloves and take a picture, only to realise I couldn’t feel my fingers. I shoved them right back in and started shaking them manically to restore some circulation. Once I could feel my fingers again, I continued my onward journey to reach the top and be treated to a staggering, celestial, 360-degree view of 120 Himalayan peaks – the closest one can be to finding salvation. The sight of such mountains resolves all anxiety. This was our heaven to find and make in the midst of our mundanities. To dwell in its beauty and be free from our earthly cravings. After munching on a few protein bars, we sat in silence and reached out to the far side of our thoughts. Paradise was finding wonder in that moment. We prayed homage to Mount Everest and descended quickly because the water we had carried up to drink had frozen over.
I later found out that George Everest had no direct connection with the mountain that bears his name, which he never even saw. He was, however, responsible for hiring Andrew Scott Waugh, who made the first formal observations of the mountain, and Radhanath Sikdar, who calculated its height. In March 1856, Waugh wrote to the Royal Geographical Society to announce that the mountain was believed to be the highest in the world and proposed that it be named “after my illustrious predecessor.” Everest’s name was used as a compromise owing to the difficulty of choosing between multiple local names for the mountain. George Everest initially objected to the honour, as he had had nothing to do with its discovery and believed his name could not be easily written or pronounced in Hindi. That is why the Nepalis still call it Sagarmatha.
We returned to Kathmandu two days later and showered after what seemed like ages. Hot water suddenly seemed like a luxury. I gorged on burgers and fries and all the meals after that made up for the few thousand calories we had lost surviving on thinned-out air. We strolled the streets of the vibrant city which made us feel like it was Goa in the mountains. A few of us opted for the invigorating Trekkers Massage in one of the tree-covered streets of the city. We feasted in rooftop cafes and got a feel of the local nightclub. We went as friends and returned as family. We went with more head on the hair and returned with more hair on the face. When I returned home, my children refused to recognise me with my beard.
I took along with me Pico Iyer’s latest book, The Half Known Life: In Search of Paradise, because that, in essence, was the purpose of our visit. Iyer chronicles a lifetime of pilgrimages with soulful curiosity ruminating on the transience of things, on the transience of us, reflecting on “The thought that we must die … is the reason we must live well. The fact that nothing lasts, is the reason why everything matters. The beauty of travel is that a visitor can see graces in a place that locals take for granted.”
Her fortitude, her belief, her prayer and unstinting love have spurred many a medical miracle. On mother’s day, we celebrate the gift that doesn’t stop giving.
When I was a resident in my final year of training at the Christian Medical College in Vellore, a malnourished lady onerously walked into the emergency carrying her 6-year-old child in her arms. Blood pouring out from his lacerated scalp had soaked them both. He had been run over by a car close to the hospital, and rather than wait for a ride, she had simply picked him up and run to us. He was unconscious when we saw him. She looked like she was going to follow suit. The ER doctors expeditiously plugged in an intravenous catheter and shoved a tube down his throat to protect his airway, while I pressed on his head with a dozen Gamgee pads to control the bleeding. Once we got the blood pressure up and stabilized his heart, we rushed him for a CT scan. The temporal bone was shattered into pieces and beneath it was a large extradural hematoma, a blood clot between the bone and the dura mater. The underlying brain, however, looked surprisingly okay.
We took him straight to the OT and cleaned out all the debris and rubble of the road from his skin, the stench of dried blood permeating through our masks. We fashioned a skin incision to expose the fractured bone and removed all the pieces. There was a large hematoma underneath the fractures pressing on the brain, which we slurped out in our suctions, and I coagulated the artery that was slit by one of the sharp fracture fragments. For that kind of injury, I was surprised to find the dura intact.
The dura mater, Latin for tough mother, is a thick durable membrane that covers the brain. The dura mater is the mother of the brain: mater, rooted in the universal maa, means mother. The primary function of the dura, akin to that of a mother towards its child, is to protect the brain – and what a fabulous job it does of that. Like a mother for her family, the dura guards the brain’s internal environment.
We put back the pieces of bone like a jigsaw puzzle and neatly sutured the scalp over it. As we wheeled him out, his mother stood there with her anxious hands folded in appreciation. He gained consciousness after a few days and was transferred out of the intensive care. She nursed him with love, feeding him, turning him, and exercising him to ensure he was on his way to a full recovery. Every time I walked into the ward, whether it was in the middle of the night or early hours of the morning, she was awake next to him, one hand of hers literally on his pulse. She took him home walking two weeks later. “A mother never outgrows the burden of love,” said the famous writer Florida Scott-Maxwell, “and to the end she carries the weight of hope for those she bore.”
The deepest grief is also borne when a mother loses a child. One of my closest friends gave birth to a stillborn child, and I held her hand as she had to let go of the life she had loving nurtured within her for months. I lost one of my best friends in a bike accident at 18; his mother’s womb was so scarred by the loss that she developed uterine cancer a few years later, which she’s overcome with the mettle of a mother. One of my mother’s friends lost her beautiful son in his forties to stomach cancer that showed up out of the blue and consumed him in a matter of months. Another of my friends was recently operated for a ruptured appendix and he never woke up after surgery; his mother’s earnest plea was for her to pass before he did, but she is still braving his passing. “Life doesn’t offer happy endings; only the prospect of finding happiness in the midst of endings that will seldom be simple,” I once read somewhere.
If given a chance, any mother would be willing to interchange and take upon herself an ill-fated outcome her child must go through. In a book I was reading the other day, the sole survivor of a plane crash was a little girl whose mother had completely wrapped herself around her. The 4-year-old child was found alive under her mother’s scorched remains. Nature has its own rules.
I vividly remember the time when my own mother had Guillain-Barré syndrome, a viral affliction of the nerves which paralysed her neck down. She was in the ICU, on a ventilator for a few weeks, with everyone involved in her care uncertain if she would make it. Her then 80-year-old mother would trek valiantly each day to the hospital and sit in one silent corner of the waiting room for 12 continuous hours only to return home to attend to her ailing husband. She wasn’t unsettled about whether her daughter would make it and she didn’t question the doctors even when she was given the same discouraging news every day for many days. “I have faith in my God, and I know he will watch over us,” she used to tell me when I asked her why she didn’t look worried, while I trembled with sorrow, bewilderment, and fear myself. She was a stoic lady, having suffered the unsurmountable loss of her first daughter a few decades ago in the infamous Handloom House fire of 1982, and was now on the brink of losing the second one. My mother survived because of her mother’s certitude. When my mother eventually lost her mother, it was the cataclysm of a lifetime.
While more phone calls are made on Mother’s Day than any other day of the year, and phone traffic spikes by as much as 37 per cent on this one single day, let us take some time on this day of joy and celebration to remember the mothers who might not receive that call or the children who have no one to make that call to. “Grief, when it comes, is nothing like we expect it to be,” Joan Didion observed in her classic meditation on loss.
So, to all the mothers who’ve been through an unfathomable illness or the fading of a child, be gentle and more generous with yourselves. You did more than your duty. To every child who has been through an abysmal illness or the passing of a mother, be grateful to the time you spent together and help carry her legacy onward.
And on a lighter note, if you’re Parsi or Punjabi, Greek or Jewish, don’t worry – your mother will never leave you. Even if you want her to. It’s a matter of lifelong complexity.
The next time you’re driving watch out for the road crossers
I used to ride a bicycle to work during COVID, but the electric buses creep up on you with such deafening silence, I’ve nearly been killed a couple of times. So now, I just drive everywhere. And when I drive with my daughters and their cousins, there is always banter about the choice of music that should be played. I try to introduce the classics to them, while they want me to listen to Blackpink, Taylor Swift and Harry Styles. “Have you ever heard of the Beatles?” I asked them, putting on ‘Hey Jude’. One of the six children in the backseat perked up. “Oh yes – it’s what old people listen to!” she retorted, while the rest of them yelled “Roasted!” in unison. In retaliation, I made them listen to Jagjit Singh’s ghazals on the way back. They may have roasted me, but I let them simmer on a slow burning flame.
Driving in Mumbai not only allows you to experience the entire spectrum of emotions the human heart is capable of fathoming but also unleashes distinct categories of ‘road crossers’ that one has the pleasure or pain of encountering. They are their own traffic signal. They have no regard for anyone around. I’m sure you’ve met all seven of them but let me give you a formal introduction.
The Hand Raiser
These are people whose brain sends them a random signal to cross the road irrespective of where they are standing. It’s often in the midst of moving traffic and nowhere close to a traffic light. The brain also simultaneously alerts the hand to be raised, as if to hail Hitler, and it remains upright until its owner has successfully completed their journey to the other side of the road. Note that there won’t be any eye contact involved. These individuals don’t care about the speed of the oncoming traffic or how many people swerve or screech to protect their life; their hand is their personalised stop sign.
The Cell Phone User
They cross the road with their head buried in their phone or while speaking on it. They belong to an alternate universe oblivious of anything known as vehicles around them. They walk around the city as if they are in a matrix playing Packman on a galactic scale. They seamlessly bump into fellow cell phone users and two or four wheelers and carry on as if nothing ever happened. They might be transiently alerted by a loud horn, but after looking up briefly and realising they are still alive, they plunge themselves back into their phone. I sometimes wish the bonnet of my car would automatically open and gobble them up to make this Packman seem a little more real.
The Tobacco Mixer
You need to keenly look out for this type. These guys must have such a busy schedule that they decided to pour out the 3-4 ingredients that go into mixing tobacco into their palms, grinding their thumb against it and placing it into a pocket of their mouth, all while crossing the road, often at a traffic light. In those who have completed this process, you are sometimes fortunate to witness the release of contents in the form of a volcanic eruption from their mouths right in front of your car. Jai Maharashtra.
The Sprinter
This is an unusual kind of road crosser. You can spot them from a distance and can register that they are waiting to cross the road. But they are extremely still. Their decision-making skills seemed to have been hacked by the Hand Raiser. You drive on with the understanding that they won’t attempt to cross until you pass, but they suddenly decide to do so when your car is one foot away from their body. They sprint across the road like a gazelle being chased by a lion in the savannah and you are forced to screech to a halt, at the mercy of being rear-ended by whoever is behind. Whether you suffer a whiplash is immaterial; the gazelle has disappeared into the bushes.
The Baby Dragger
These are parents accompanied by children who inevitably refuse to cross the road when the pedestrian light turns green. These children are either too heavy to be carried or too light to cross on their own. When it’s time to cross the road, the first few seconds are spent in cajoling and requesting the child, the next few are spent threatening it, and when only ten seconds remain and it’s do or die, the parent loses all patience and the poor baby is dragged with an outstretched arm – like airport luggage that you can’t carry or push and there is no trolley around. To know if you were dragged as a child, stretch out both arms in front of you and check if one of them is slightly longer. You really fell for it, didn’t you?
The Undecided
These are perpetually confused about whether they should cross or not. They take two steps forward and four steps back. They are uncertain of their ability to dodge ongoing traffic. They stop and move in random patterns, causing all the cars around them to do the same. And after all that chaos, they most often end up on the same side of the road. They most probably simply want to add some spice to the lives of those who are sitting stuck and bored in traffic. For their own sake, they should hold hands with the Sprinter.
The Vendor
The real intention of these people is never to cross the road at all but sell you stuff like singh-chana at a signal or in the midst of briskly moving traffic on the Western Express Highway. The skill with which they do it, without disrupting traffic and allowing for buying, selling, and bargaining at 25 kmph is only possible in this part of the world. They are prolific road crossers who can not only traverse four lanes of a moving expressway but make a business out it.
All of us need to get somewhere every day, and we each have our own way of doing so, whether it’s by driving or walking. We are fortunate to live in a maximum city where we can derive joy from the most minimum of pleasures, like watching how one chooses to cross a road and not having run over anyone yet. For that, I am grateful.
When a doctor steps out of the hospital frenzy, and finds himself in the thick of a chaotic celebration of food and customs
It was one of my fervent desires to experience the essence of Mohammad Ali Road during Ramzan, and so, a few days before Eid, a bunch of us from the hospital decided to show up there amidst organised chaos. We walked past pop-up stalls selling copies of every famous brand under the moon betwixt the jarring honking and dodgy manoeuvring of two and four wheelers, whose drivers’ fingers seemed to be badly glued to their car horns. I remember thinking that if we could navigate that road at 10 PM at night, we had a serious shot at auditioning for the Cirque du Soleil.
Through some dilapidated shops we went, making our way through some of the finest craft work, intoxicating perfumes, and dry fruits and extremely alluring nuts. Our destination was the Khau Galli that starts at the Minara Masjid, a beautifully verdant mosque lit up with ornate lights that herald the arrival of all things beautiful. As we got to the entrance of that lane, I was mesmerised. The crowds had doubled, the shops had tripled, and the sights, smells. and sounds had quadrupled.
I felt like I was in one those movies when they depict a man tied in a trance with the universe moving around him at a whirlwind speed. In the middle of being surrounded by a few thousand people, I felt a push with someone shouting into my ear, “Tera dhyaan kidhar hai? Maal toh idhar hai!” For a moment, I wondered if I was in the wrong lane with some dubious activity going on, until he held my hand and placed a plate of malpua on it. That’s when I realised that the maal he was referring to was a food item. For the uninitiated, malpuas are small pancakes made with flour that is deep fried in desi ghee or refined oil and then soaked in sugar syrup – a perfect ditch to the start of my low carb week. We crammed in a few with the ghee dripping off our fingers, and when we asked for some tissue, our server pulled out a sheaf of newspaper, stating, “Indian tissue.” After confirming it wasn’t the Sunday Mid-day and then wiping our hands dry, I signalled asking him where I could dispose of it, and he pointed to the ground. “Indian dustbin?” I asked and we both nodded our heads and smiled, as I put it in my pocket to discard later.
We needed to walk a little to digest our starter, which should have ideally been dessert. We walked, or rather simply stood, while we were being gently displaced past exotic shawarmas roasting on a slowly turning vertical rotisserie, as the guy sliced thin sheets of the meat which were then rolled into a flatbread and served amidst constant chants of “Chalte raho!” by the public. The fragrance of multitudinous meats being roasted all around me was invigorating to the senses. Every conceivable succulent kebab in every imaginable colour stood skewered on sticks besides full-blown chickens ready to be barbequed or whatever else they do with them.
We turned left into one of the dendritic lanes where the food turned even more exotic. Brains (bheja), kidneys (gurda), and livers (kaleji) were kept boiled on plates for display. As a brain surgeon, I was faced with a predicament: Was it appropriate for me to consume the very organ I treat on a daily basis? I wondered if a urologist would be amenable to eating a kidney or if a hepatic surgeon would devour a liver. Before I was able to process my dilemma fully, we were huddled onto a few stainless steel stools. Yellow plastic plates with the organs cooked in a piquant masala made its way onto the makeshift tables alongside bread and roti. Sometimes, the choice is made for you and all you must do is surrender. Vegetarians, I hear you, but it was one of the most delectable meals I have ever had. We ordered some more.
Having tantalised our tastebuds, we decided to walk again amidst chants of “Kal to aap ki jaan bhi ja sakti hai, mobile kya cheez hai?” cautioning us to keep our belongings safe. It was nice to see foreigners, their Instagrams on, attempt this experience, as white skins bumped into brown and sweat was exchanged, as smoky fumes of something roasting filled the air. I overheard one of them say, “Until now, I only thought that if you can drive in India, you can drive anywhere in the world, but now I feel that if you can walk on this street, you can walk anywhere in the world!” They had big smiles on their ‘go with the flow’ faces as they kept taking pictures with one hand above the heads in the crowd.
We passed by shops with colossal vessels, in which hundreds of kilos of biryani was being dished out. There were cutlets and rice cakes, egg rolls and the famous nalli nihari – marinated lamb with a zoo of spices. After gorging on as much as we could, we decided it was time for dessert. We lapped up the kesar phirni served in earthen clay bowls, chomped on a few golden jalebis, and ended with a royal falooda – also nicknamed Sharbat-e-Mohabbat. “We have to spread love, not hate,” I was told by a man in Urdu as he served us a chilled glass brimming over its own edge. The smooth sev mixed with ice cream in the drink soothed all the fire in the belly.
As we walked back to my car that was parked very far away, I thought how blessed we were to live in a country where we can celebrate a multitude of religions and cultures with such wholeheartedness.
Where we can seamlessly partake in each other’s joys and ritualise each other’s customs.
Where we can gourmandise each other’s food and honour each other’s traditions.
Where we can do our own thing and make space for others to do theirs. Even when it involves exceedingly high decibels.
Where all we need is some Sharbat-e-Mohabbat to share with each other. Let’s drink to that.
In this new monthly column Mazda explores the relationship he has with his daughters (and everyone else).
“What would you like to be when you grow up?” I asked my daughters the quintessential question that all parents ask their children eventually at some point. My daughters were on the back seat of our car as we drove in the chimeric traffic of Mumbai to hopefully someplace nice. My elder daughter, Meher, is a little more than 8 years old, and my younger daughter, Khursheed, is a little less than 7. Just like in every other family where children are brought up by the same parents in the same environment, they too are poles apart.
“I wanna become a make-up artist… for dead people,” Meher, who spends a large portion of her day in front of the mirror, said unflinchingly. I screeched on the breaks but not from her answer; that’s how one spends Sunday evenings if going towards Bandra. “Why should people who have died not look pretty?” she wondered aloud. “Plus, unlike with alive people, I can do whatever make-up I think looks good and they won’t fuss!” she made her point. “Alive people have too many issues,” she concluded rightfully amidst all the unnecessary honking that people around us were indulging in.
“Maybe we should get you a vacation internship at John Pinto,” I proposed, “and instead of going for summer camp or learning how to swim, you could learn how to make dead people look good.” “Pinto!” she exclaimed, giggling at the name. “They take such good care of people that some of them look better dead than when they were alive,” I joked. “When someone dies, they clean them up, put make-up, dress them up in a suit or saree, and put them in a fancy coffin where they can be buried looking fresh and happy,” I said smilingly, as I swerved to miss hitting an erratic two-wheeler. “Careful, Dadda, don’t kill him – I don’t have my make-up kit with me!” she joked.
“You could also learn the art of embalming,” added my wife sitting next to me, who is pursuing her hypothetical master’s in ancient Egyptian techniques. “That’s the real make-up!” “What the heck is that?” Meher asked. “When someone dies, the body is preserved by injecting certain chemicals in it to dry it up and make it look fresh for many years, so there’s not much decay. It’s a very tough process to master,” she tried to explain simply. “It’s also called mummification,” I interjected. “I wonder why,” Meher mused. “It’s because all daddies want their children’s mummies to look fresh even after many years!” I added, and promptly got a slap on my thigh from my wife. I did later find out that ‘mummification’ comes from the Arabic word mummiya, a substance that was first used in the preservation process.
“I wanna become a teacher,” said my younger one, looking out of the window as she loves to do every time we go for a drive. “Because all the teachers in my school are really kind,” she went on to answer without even being asked why. “Today in English, we learnt prep… something (her six-year-old self was trying to figure out how to say ‘prepositions’) and teacher made us play a game to learn it simply.” “Give me an example,” I said. “Like miss asked us to put our bags on the table… so ‘on’ becomes the prepopittin or whatever it’s called, she said, smilingly hushing away her struggle. “Then she asked to remove our lunch box from the bag and eat whatever was in it… so ‘in’ is the prepsitition,” she continued, shaking her head and shaking away her inability to pronounce it. “Okay cool, let’s play a game. I’ll make a sentence and you fill in the blanks when I say dash with the precipitation or whatever that word is,” I levelled up. I haven’t seen kids this excited in Mumbai traffic before.
“Tina sat dash Tom,” was the first thing that came to my mind, and they started giggling out loud. I wondered why and only after a few seconds did I realize that their single-digit minds were naughtier than my double-digit experience. “Okay, let me give you a clue: it’s not ‘in’ and it’s not ‘on’!” I announced, suddenly wiping the smiles off their faces. They didn’t have an answer for a few seconds until Khursheed raised her hand on the back seat and said ‘behind’ as though she was still in class. “Thank God, or else, I was going to make a call to your teacher,” I said, giving them a fake stare. “The answer could have even been across or near or besides,” I went on, wondering to myself if these were actually prepositions. The beauty of having school-going children in the first and second standards makes you realize how little you know. But I take solace from the fact that there is no point in knowing so little.
We finally reached our destination. The conversations I have with my kids makes traffic seem interesting and that much more meaningful. I love talking to children, mine and everyone else’s. They are unfathomably wise and I believe we have a lot to learn from them. Their minds are not constrained by the realm of reality and each of them is a fulcrum of wonder. They silence your rationality and make you believe in magic. It’s a pity that they have to grow up. But until they do, stay tuned to this column for more.
For patients and their relatives, waiting for answers can be both unnerving and exhausting
“How long will surgery take?” a family of four nervously asked me outside the operating room, as I prepared to walk in to remove a jumbo brain tumour from their matriarch. “It’ll be about 4-5 hours, but don’t be surprised if we finish earlier or get worried if we take much longer,” I cautioned, always giving myself some room so that relatives don’t panic. “It’ll depend on the consistency of the tumour and the ease with which we can peel it off the internal carotid artery, which is the main blood vessel encased completely by the tumour and supplying blood to half the brain,” I explained.
“All the best,” they said, apprehensively. “Don’t worry, everything will be fine,” I signed off with the trademark sentence I give every family before disappearing into the mysterious world of the operating room, the sanctum sanctorum of every surgeon.
Once there, we studied the MRI in detail again as the anaesthesiologist effortlessly put the patient to sleep. We fixed the head on a clamp to stabilize it and then turned it to give us a straight trajectory to the tumour, locking it in the final position. I shaved a strip of hair behind the hairline and marked our incision site with a marker. Then, I cleaned the area with a combination of three differently coloured solutions to sterilize it and allowed for it to dry. Finally, we draped the patient in the usual fashion by neatly arranging wires, instruments, and suction devices, ready to start surgery.
Within the hour, a nurse walked in with a message. “The relatives are asking if everything is going well,” she said. “Tell them we’re just about to start,” I said, a little irritated, especially when I needed to be in the zone. “Also tell them, gently, that I will come out and talk to them once it’s over,” I course corrected.
I made a curvilinear incision behind the hair line and retracted the scalp to bare the bone. We drilled a few starry holes in the skull and cut off the bone in a shape resembling an almost perfect constellation of Orion. For the next hour, we drilled the bleeding bone down to the base of the skull, flattening all the ridges that looked like a mountainous terrain. Just as we were about to open the covering of the brain, the dura, another nurse came and mumbled something in Malayalam, her voice muffled by the sound of the drilling. “The relatives want to know, how much more time?” “Ask them to have breakfast and then some lunch, sister, and to come back after that. And the next time they ask, please handle it yourself because we cannot be disturbed now,” I instructed, even asking that a Do Not Open sign be put outside the operating room door.
Once we opened the dura, we saw the tumour that occupied the entire temporal lobe, displacing the brain several centimetres behind its usual position. Having disconnected its blood supply, we got into it, coring out its contents in a steady and meticulous fashion. We then went under the frontal lobe to remove the portion that had crept through. We spent the next 2 hours separating the tumour from the carotid artery and optic nerve, which it had straddled, in very slow and precise moves, because one wrong cut could be catastrophic.
“Sir, the relatives are crying outside,” one sister came in frantically. “They want to see you.” I looked at the clock and realised with surprise that it was already 6 PM; we had lost track of time and space. “It is we who are passing when we say time passes,” I remembered a quote from French philosopher Henri Bergson. “Tell them that surgery is over and everything went well,” I announced, as I removed the last piece of tumour and closed back everything the way we usually do it.
I walked out to meet the relatives, who looked like they had gone to war. I calmed their anxious nerves, explaining to them why surgery had taken longer than expected, but they were relieved only when they saw their mother being wheeled into the ICU fully awake, telling them she was okay.
Until that day, I had never stopped to wonder what waiting patients go through – outside the operating room, ICU, or even a doctor’s office. The chief surgeon with whom I trained in the United States, when asked how long surgery would take, always told relatives, “It’ll take as long as it does,” and never gave a timeframe to probably mitigate the family’s anxiousness. We in India offer a more emotional response. I, at the very least, give my patients as much information as I can because I simply cannot fathom what they must be going through, waiting without any idea. However, I get some sense of that desperation when patients take longer than usual to wake up and gain consciousness after brain surgery. I believe no patient or their relative will ever be able to gauge the myriad thoughts and emotions a surgeon goes through in that brief period of waiting, which seems to stretch as long as eternity.
Outside every ICU of every hospital there are relatives who wait for their loved ones to be shifted out. The lucky ones wait for a day, the unfortunate ones wait for weeks or even months. Day after day, we shower people with various bits of information that we don’t know how much longer it’s going to take, whether it’s for someone to wake up or for an infection to subside or for a swelling to resolve or for someone to come off the ventilator. But there will always come a time when the wait is over. Oftentimes, it’s in our favour; sometimes, it isn’t.
In some sense we are all waiting. But it is important to remember, as the famous American professor Jason Farman once said, “Waiting isn’t a hurdle keeping us from intimacy and from living our lives to our fullest. Instead, waiting is essential to how we connect as humans.”
If you’re a parent, you’re waiting for your kids to go to school, and then you’re waiting for them to come home every evening. If you’re a housewife, you’re waiting for the maid to show up. If you have a corporate job, you’re waiting for the weekend. If you’ve lost a job, you’re waiting to find another. If you’re pregnant, you can’t wait to deliver. If you live in America, you’re waiting for July. If you live in Mumbai, you’re waiting for January. If you live in Canada, you’re simply waiting. Some are waiting to win the lottery. Some are waiting to move into their promised redeveloped buildings. If you’re single, you’re waiting to be married. If you’re married, you’re waiting to be single again. If you have five senses, you’re trying to cultivate the sixth. If you’re in the 10th, you’re waiting for your exams to get over. If you’re in the 12th, you’re waiting to prepare for the next entrance exam you have to take. Some are waiting for the war to end. Some are waiting for the stock market to go up, while some are waiting for it to go down. Some of us are waiting to climb Everest. Some of us are waiting to go deep sea diving. Some are waiting for their next meal. Some are waiting for the next messiah to save the planet.