Why it’s important for a doctor to be part of a team whose decisions are constantly questioned, and healthy dialogue is the order of the day.
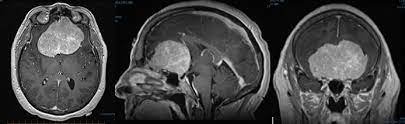
 “Why can’t we have some surgeon-friendly anaesthetists?” I questioned my anaesthetist, who had bellowed back at me for asking her to hurry up amidst her getting my patient ready for surgery. “I need to secure an extra intravenous line, and an arterial line since we are turning him prone,” she started explaining, ending with “…why can’t we have more anaesthetist-friendly surgeons instead!” rolling her eyeballs almost up to the ceiling. I could see condensed air emanating from the sides of her mask, the silent gestural interpretation of having to put up with a surgeon’s low IQ. To infuriate her even more, I retorted, “It’s just a simple cervical laminectomy!”
“Why can’t we have some surgeon-friendly anaesthetists?” I questioned my anaesthetist, who had bellowed back at me for asking her to hurry up amidst her getting my patient ready for surgery. “I need to secure an extra intravenous line, and an arterial line since we are turning him prone,” she started explaining, ending with “…why can’t we have more anaesthetist-friendly surgeons instead!” rolling her eyeballs almost up to the ceiling. I could see condensed air emanating from the sides of her mask, the silent gestural interpretation of having to put up with a surgeon’s low IQ. To infuriate her even more, I retorted, “It’s just a simple cervical laminectomy!”
“There’s no such thing as just a ‘simple’ surgery… you know this better than I do!” she exclaimed, reminding me of my own neurotic obsession to fuss about the tiniest and most frivolous detail in every single operation. “He has a bad heart; you know that, right? We’ve even taken a DOT consent. “What’s DOT?” I asked, not being a fan of abbreviations. “Death. On. Table!” she said, with a short, emphatic pause after each word. This time, my eyes reached the ceiling and came rolling back. “You surgeons don’t see anything apart from the organ you’re operating on, right?” she went on, putting the final taping to secure all her paraphernalia. “Of course we do,” admitting to myself quietly that we often don’t. “We’ve even got fitness for surgery from the cardiologist,” explaining my diligence. “Fitness for surgery is a meaningless term. Anyone who can lie down is fit for surgery. Fitness for anaesthesia is what’s needed,” she retorted, having used that line umpteen times before, borrowing from something she had once read somewhere.
In today’s age, every specialist looks at a patient from their point of view. I have to make sure I can surgically relieve him of his pain. The cardiologist has to ensure that his heart is optimized to withstand the operation. The physician checks that his blood sugars and blood pressure are stable. The anaesthetist has the ultimate responsibility of navigating the ship through the storm if something were to happen, and hence the excruciating emphasis on safety. “The cause for multi-organ failure is single-organ doctors,” one of my teachers used to say, emphasizing the need for being holistically involved in treating a patient.
I remember once operating on a patient’s lower back because he could hardly walk a few steps, having been debilitated by pain for years. He had severe lumbar canal stenosis. The operation relieved his pain completely, and in his newfound freedom and excitement, he started walking several kilometres a day until he had a heart attack. The heart was not conditioned to withstand such a drastic change in such a short span. Luckily, this was not a classic case of ‘the surgery was successful, but the patient died’; this man was okay with one stent placed in time.
After we were given permission to advance with the current case at hand, we flipped the patient nervously on his belly and continued to proceed with the cleaning and draping of the patient in the usual fashion, but this time, the corner of one eye was constantly on the monitor, checking for any fluctuation of heart rate or blood pressure. “If his heart stops, we’re not going to be able to resuscitate him in this position, with him lying on his stomach and his head fixed rigidly on a clamp,” were her soothing words just before I sliced into the back of his neck. To keep up with her wit, I stated mid-way through surgery, “We are losing a lot of blood, hope you’re okay there!” In reality, we were in control; I simply wanted to make sure she was glued to the right screen. We removed the compression meticulously, ensuring the spinal cord was pulsating gently. We were done before the anaesthetist could say anything else to us. But I was wrong; she wasn’t finished.
“Why did you book the case for 6 hours if you could finish it in 2?” she said, smiling behind her mask. “I included the time you would take to get the patient in and out of anaesthesia,” I teased, dismantling my gloves in the heroic fashion surgeons do when they finish a successful operation.
Doctors tend to view patients from different perspectives. Two surgeons viewing the same problem may have a completely different outlook because of context and relativity. A famous spine surgeon once said, “Anyone with a spine problem can be managed without surgery and anyone can be operated; there are very few absolutes.” It is for this reason that the more opinions a patient takes, the more confused they end up being. Medicine is an ambiguous science, leaving those dealing with patients’ lives in a constantly elusive quest of what is the right thing to do.
Two senior physicians may argue on whether a patent is optimized for surgery based on sound reasoning from the information at hand and may yet arrive at varying conclusions. Neither is right or wrong; the knowing is always in the doing, or sometimes, in not doing. On occasion, doing something has a price to pay, but so does not doing it. The best – and worst – part is, we always have a choice. Recently, we were reluctant to operate on someone for a spine issue without optimizing him because we felt the risk from his compromised heart function was too high. The patient was operated immediately elsewhere – successfully.
I’m fortunate to be part of a team where my decisions are constantly questioned. Where patient safety is a prime concern but there is still a willingness to push the envelope. Where we have to perpetually engage in dialogue – sometimes gentle, sometime harsh. Where we have to explain why we want to do what we need to. It’s strange that we are all fighting for a common goal, which is the good of the patient, and yet, everyone has a different perspective of what ‘good’ is.
After all, as the famous saying goes, “No one sees what you see, even if they see it too.”